
Laryngoscopy is an exam that lets Drs. O’Halloran, Egan, and Scheidemandel see the back of your throat, your voice box (larynx), and vocal cords using a tool called a Laryngoscope. A Laryngoscopy will be performed for the following reasons:
There are two different types of laryngoscopy – Indirect and Direct.
This procedure is done in the office using a small hand held mirror at the back of your throat. You will be asked to sit up straight, stick out your tongue and possibly make some eee or ahhh sounds while Drs. O’Halloran, Egan, and Scheidemandel shines a light in your mouth to reflect the light to the back of your throat. Advances in technology have made this type of procedure less common. We most often use a flexible laryngoscope instead which lets us see your throat better and it’s more comfortable for you.

Direct laryngoscopy lets us see deeper into your throat with a fiber-optic scope. There are rigid scopes, which are often used in surgery to remove foreign objects, perform biopsies, remove polyps or perform laser treatments. It may also be used to help find cancer of the voice box. Rigid scopes are used under general anesthesia.
In the office, we use a fiber-optic scope, which is thin and flexible and enables direct access to your throat. First, you may be given a numbing spray and/or a medication to dry up the secretions in your nose and throat. Then Drs. O’Halloran, Egan, and Scheidemandel will put the scope through your nose and gently down your throat.
For the in-office procedure using a flexible scope, please do not to eat or drink anything before the procedure. Although numbing medication is used, some patients with a strong gag reflex may have trouble and we want to prevent vomiting. If you wear dentures, you will just need to remove them before the examination.
If a rigid scope is necessary, it will be performed under general anesthesia. Drs. O’Halloran, Egan, and Scheidemandel will want to know if you:
Have had surgery or radiation treatments to your mouth or throat
Prepare as you would for a surgery. Be sure not to eat or drink for 8 hours before the procedure. Remove all jewelry, dentures, glasses, and use the restroom. Also plan to have someone drive you home following the procedure.
Once you are asleep, Drs. O’Halloran, Egan, and Scheidemandel will place the scope in your mouth and down your throat to perform your treatment. The exam will take approximately 15-30 minutes. After the procedure, you will be in recovery until you are fully awake and able to swallow.

Tonsillectomies and adenoidectomies are common and safe procedures. As a matter of fact, tonsillectomy is the second most common pediatric surgical procedure. It is also necessary at times for this procedure to be performed on adults. A tonsillectomy and adenoidectomy can help prevent frequent sore throats and ear infections. These procedures are not always performed at the same time. Only one may be needed, sometimes both.

The tonsils are glands located in the back of the mouth on both sides of your throat. As part of the immune system, tonsils help fight infections. The adenoids are located behind the soft palate, the back, muscular section of the roof of your mouth. Adenoids also help fight infections. Behind the uvula, there is a passageway that connects the nose to the mouth. And in this passageway, the eustachian tubes connect the middle ear to the back of the nose. These tubes prevent large differences in pressure inside the ear. When your adenoids swell, they become inflamed and can cause blockage of the eustachian tubes. Blockage can cause your middle ear to become filled with pus, causing additional infection and swelling. This can even lead to hearing loss.
Tonsillectomy is generally performed because of repeat occurrences of tonsillitis. Tonsillitis is an infection in the throat that starts with your tonsils. These types of sore throats are usually severe and fever can occur. It hurts to swallow!
It’s important to be examined when you have tonsillitis because it’s can be dangerous if there have been five or more occurrences within one year. And when the illness is not responsive to antibiotic treatment, please see us immediately!
Additionally, if your tonsils get large enough to touch each other you probably have a serious case of tonsillectomy. Also, if there is an abscess surrounding your tonsils, you will see puss filled sacs. This is another cause for attention.
Treatment of tonsillitis and ear infections generally requires antibiotics. If left untreated, tonsillitis could damage organs in your body. Tonsillectomy is a procedure in which the tonsils are removed. Adenoidectomy is a procedure in which the adenoids are removed. The combined operation is called a T&A. Generally these surgical procedures are performed if antibiotics are unresponsive. If antibiotics do not work to eliminate tonsillitis or ear infection, a tonsillectomy and possible adenoidectomy may be performed. These surgical procedures will help you reduce the number of throat and ear infections.
Tonsillectomy and Adenoidectomy is performed under general anesthesia. Drs. O’Halloran, Egan, and Blank can remove the tonsils and/or adenoids in many different ways. Traditional surgery requires the use of a scalpel. Some surgeries respond better to a laser. When surgery is complete, bleeding is stopped and the patient is admitted into recovery. Upon awakening, you will be given pain medication. Within a little while, you will be able to go home. Surgery is usually well tolerated although a sore throat is common for the first 5-10 days after surgery. Watch for bleeding. You will initially find it easiest to swallow liquids and cold desert like foods.

A deviated septum is one of the most common reasons to have non-cosmetic nasal surgery. Your septum can be crooked and may result in a smaller nasal passage on one side or the other, or even both. In a normal nose, the mucosal lining swells and retract many times a day. With a deviated septum, one may have difficulty breathing from either side of the nose. It is usually from the already small passageway being blocked further from the swollen mucosal lining. Sometimes, blockage can occur when there is additional cartilage, bone or mucosal tissue.
This difficulty in breathing through the nose could be corrected through a Septoplasty. Many people breathe loudly and others think their noses are stuffed, but in fact they suffer from a deviated septum and when their tissues naturally swell, the side with the deviation is even more restricted
A Septoplasty is the surgical procedure to straighten a deviated or crooked septum to improve breathing, function, and minimize possible sinus infections, creating greater comfort for the patient. A septoplasty is almost always performed with no visible incision and normally takes about 1 to 1 1/2 hours. If the Septoplasty is being performed in conjunction with a Rhinoplasty, there may be additional, visible incisions and may take about an additional hour or more for difficult cases.
A Deviated Septum is by far the most common reason for non-cosmetic nasal surgery. Your Septum can be crooked and result in a smaller nasal passage on one side or the other, or even both sides! The mucosal lining of the nasal passages normally swell and retract several times during the day. If someone with severe or a minor deviated septum experiences difficulty breathing, it is usually from the already small passageway being blocked further from the swollen mucosal lining. Its amazing that many people who go through their entire lives may never know that their difficulty breathing through the nose could be corrected through a Septoplasty!
Turbinate reduction is commonly performed in conjunction with Septoplasty to improve the nasal airway and reduce congestion. We use the Medtronic Inferior Turbinate Blade to provide minimally invasive reduction of turbinate hypertrophy. Scientific evidence shows this technique to have superior long term results and minimal complications versus other approaches. Dr. O’Halloran devised the technique described and invented the patented Medtronic Turbinate Blade seen below.

See a video showing the Inferior Turbinate blade in use demonstrating it’s minimally invasive nature which preserves the overlying mucous membrane.

Sinus Surgery is one of the most common operations performed. Drs. O’Halloran, Egan, and Scheidemandel will review with you whether this procedure is the appropriate procedure to open possible sinus obstructions. Removal of such obstructions may require eliminating polyps that are blocking sinus openings or possibly enlarging the hole that sinuses drain through.

Sinuses are the empty pockets that are filled with air in the head. There are actually four pairs of sinuses within your skull. These circulate air while lubricating the nose. This keeps the sinuses free of bacteria, dirt, and other particles. Mucos line the sinuses and secrete mucus which traps particles from incoming air. These dust particles are then expelled via cilia, small hair like fibers. Sinuses that are in good health are not obstructed or clogged. Mucus is able to pass through into the nose and then the throat without problems.
Colds, allergies, infections or other obstructions of the sinuses (i.e. deviated septum) can cause inflammation of the mucosa and block the drainage of the sinus cavities. If the sinuses become inflamed, Sinusitis can occur. The mucos becomes thicker and cannot pass through the openings and end up accumulating in the sinuses. Many symptoms can arise including fever, headaches, and pain over and underneath the eyes. Polyps form when mucosa becomes swollen by repeated infections.
Drs. O’Halloran, Egan, and Scheidemandel will determine if you have sinusitis during your examination. He will examine your ear, nose and throat and determine the cause of your sinusitis. Diagnosis can occur with the help of x-rays, CAT scan or MRIs in order to see the sinuses within your skull. Blood or allergy tests may also be performed. Treatment may be based upon the cause of your infection. Obstructions caused by allergies can be minimize or eliminated by treating the allergy. Sometimes humidifiers, warm compress over your sinuses, or drinking lots of fluids (which thins out your mucus) can also alleviate symptoms. Medications including antibiotics can treat an infection in the sinuses and control the condition. Repeated sinusitis may be caused by an obstruction and will be most responsive to surgery.
Surgery can be performed in a number of ways. It’s possible that the walls between sinuses are removed to make the sinuses larger. When the sinuses are larger, there is less of chance for obstruction to occur. Sometimes new openings are created in the sinuses for better drainage. If an obstruction is caused by a deviated septum, surgery can help straighten it out. Many of these options are performed endoscopically and under general anesthesia. Patients usually are treated and go home the same day.
While endoscopic sinus surgery is a proven and effective technique some patients may benefit from Balloon Sinuplasty a cutting edge procedure that safely on effectively opens the sinus passages without the need for surgery or anesthesia. This can be done in the convenience of the office setting. Patients can drive them selves home after the procedure and most patients return to work the next day.
Sinus surgery is a very common procedure and helps treat sinus disorders. There are some rare risks, which should be discussed during your visit with Drs. O’Halloran, Egan, and Scheidemandel. Drs. O’Halloran, Egan, and Scheidemandel will explain possible complications to help you better understand your treatment options.
The uvula is a piece of dangling soft tissue found above the back of your tongue. It can contribute to snoring, especially in patients with elongated, large, or tapered uvulas. While sleeping, breathing may cause the uvula to vibrate, creating snoring.
An uvulectomy is a procedure Drs. O’Halloran, Egan, and Scheidemandel may recommend if you are a candidate. Candidates for uvulectomy are those whose snoring problems can be traced to the uvula. During the procedure, Drs. O’Halloran, Egan, and Scheidemandel will perform coblation therapy, which is similar to traditional laser surgery, but requires a much lower temperature. Radiofrequency energy is delivered to the uvula to gently remove the excess tissue, and open up the oral airway.
Coblation therapy for uvulectomy is performed in-office using local anesthesia, and usually takes less than 20 minutes. The noninvasive nature of the surgery ensures it produces minimal damage to surrounding cells, and most patients leave with minor discomfort. Normal activities can generally be resumed shortly after surgery.

Parathyroid surgery, or parathyroidectomy, is a procedure during which the surgeon removes part or all of your parathyroid glands.
When is it used?
There are four parathyroid glands located on the outside borders of the thyroid gland in the front of the neck.
The parathyroid glands help control the levels of calcium and phosphorous in the blood. When over-activity of the parathyroid glands develops, it is called hyperparathyroidism. This causes increased levels of calcium in the blood. You might experience muscle weakness, premature thinning of the bones, kidney stones, decreased alertness, frequent urination, and occasional joint discomfort.
What happens during the procedure?
We use a minimaly invasive procedure (MIP) for most parathyroidectomy cases.You will receive a general anesthetic. The surgeon will make a cosmetically placed incision in your neck measuring only about 2 cm in length and expose the parathyroid glands. The abnormal parathyroid gland (adenoma) is removed while leaving the surrounding structures intact. The resulting scar is barely visible and hidden in a neck crease line.
We also typically use a nerve monitoring system (NIMS) by Medtronic that allows us to help preserve and protect the nerve to your vocal cords.
What happens after the procedure?
You are usually in the hospital overnight and might go home the same day. You might have some swelling in your neck with local discomfort. Depending upon your calcium level, you might need to take additional calcium to avoid the symptoms of low calcium (occasional numbness and tingling in the extremities).
What are the benefits of this procedure?
You will no longer have high calcium levels in your blood. The abnormal parathyroid gland(s) have been removed.
By eliminating the high calcium level in your blood, you will be protected from the short- and long-term consequences of calcium elevation.
What are the risks associated with this procedure?
With parathyroid surgery, the risks are minimal but might include:
Blood loss
Infection
In addition, an occasional patient might have transient hoarseness, which is rarely permanent. Rarely, a patient might have recurrence of hyperparathyroidism as disease develops in a previously unaffected gland.
When should I call the doctor?
Call the doctor immediately if:
You develop a fever
You notice numbness or tingling in your face, lips, or hands.
Obstructive sleep apnea is a serious condition that affects 4-9% of the United States population. People with OSA have disrupted sleep and low blood oxygen levels. When obstructive sleep apnea occurs, the tongue is sucked against the back of the throat. This blocks the upper airway and airflow stops. When the oxygen level in the brain becomes low enough, the sleeper partially awakens, the obstruction in the throat clears, and the flow of air starts again, usually with a loud gasp.
Repeated cycles of decreased oxygenation lead to very serious cardiovascular problems. Additionally, these individuals suffer from excessive daytime sleepiness, depression, and loss of concentration.
To diagnose sleep apnea and other sleep disorders, a sleep study at an overnight sleep lab has traditionally been recommended. However, portable sleep monitoring devices have recently emerged to help identify disruptive sleep patterns without sacrificing your time or comfort.
Home sleep studies allow Drs. O’Halloran, Egan, and Scheidemandel to monitor your sleep patterns in the comfort of your own home, and without interrupting your normal nightly routine. The home sleep study device is generally worn on your wrist, while finger probes connected to the device gather your data and vital signs. The information is stored on a removable memory card and downloaded for Drs. O’Halloran, Egan, and Scheidemandel to analyze. Drs. O’Halloran, Egan, and Scheidemandel will then be able to recommend an appropriate treatment method for you.

Thyroid surgery is used to treat thyroid nodules, thyroid cancer, and hyperthyroidism. During this procedure, part or all of the thyroid gland is removed. The thyroid gland is a butterfly-shaped gland located at the front of the neck. During surgery, an incision is made in the skin. The muscle and other tissues are pulled aside to expose the thyroid gland.
What To Expect After Surgery
Many people leave the hospital the morning after surgery. How much time you spend in the hospital and how fast you recover depend on your age and general health, the extent of the surgery.
Why It Is Done
Surgery is used to treat thyroid problems if:
• Thyroid cancer is present or is suspected.
• A noncancerous (benign) nodule is large enough to cause problems with breathing or swallowing.
• A fluid-filled (cystic) nodule returns after being drained once or twice.
• Hyperthyroidism cannot be treated with medicines or radioactive iodine.
You may have all or part of your thyroid gland removed, depending on the reason for the surgery.
• Total thyroidectomy. Your surgeon will remove the entire gland and the lymph nodes surrounding the gland. Both sections (lobes) of the thyroid gland are usually removed.
Additional treatments with thyroid-stimulating hormone (TSH) suppression and radioactive iodine work best when as much of the thyroid is removed as possible.
• Thyroid lobectomy with or without an isthmectomy. If your thyroid nodules are located in one lobe, your surgeon will remove only that lobe (lobectomy). With an isthmectomy, the narrow band of tissue (isthmus) that connects the two lobes also is removed. After the surgery, your nodule will be examined under a microscope to see whether there are any cancer cells. If there are cancer cells, your surgeon will perform a completion thyroidectomy.
• Subtotal (near-total) thyroidectomy. Your surgeon will remove one complete lobe, the isthmus, and part of the other lobe. This is used for hyperthyroidism caused by Graves’ disease.
How Well It Works
Success of a thyroidectomy to remove thyroid cancer depends on the type of cancer and whether it has spread (metastasized) to other parts of the body. You may need follow-up treatment to help prevent the cancer from returning or to treat cancer that has spread.
Risks
Thyroid surgery is generally a safe surgery. But there is a risk of complications, including:
• Hoarseness and change of voice. The nerves that control your voice can be damaged during thyroid surgery. This is less common if your surgeon has a lot of experience or if you are having a lobectomy rather than a total thyroidectomy.
• Hypoparathyroidism. Hypoparathyroidism can occur if the parathyroid glands are mistakenly removed or damaged during a total thyroidectomy. This is not as common if you have a lobectomy.
What To Think About
If you have a total thyroidectomy, you will develop hypothyroidism and need to take man-made (synthetic) thyroid hormone for the rest of your life.
You will most likely be treated with radioactive iodine after surgery for thyroid cancer to make sure that all the thyroid tissue and cancer cells are gone.
You may have a lobectomy, with or without isthmectomy, if your doctor suspects that a nodule may be cancerous. If you do have cancer, a surgeon usually will do a completion thyroidectomy.
After surgery for hyperthyroidism, some people will have low calcium levels and may need to take calcium supplements.

A clinically proven, minimally invasive technology for treating chronic sinus inflammation without the need for surgery or anesthesia. The Balloon Sinuplasty™ system by Acclarent™ uses a small catheter and balloon to quickly open and expand blocked sinuses.
Sinusitis is one of the most common chronic health problems in the U.S., afflicting 37 million Americans each year. Patients suffer headaches, congestion, fatigue and other symptoms. This condition significantly impacts an individual’s physical, functional, and emotional quality of life.
Historically, sinusitis patients were limited to two treatment options: medical therapy such as antibiotics and topical nasal steroids, or conventional sinus surgery such as Functional Endoscopic Sinus Surgery (FESS). Medical therapy can help alleviate symptoms as many as 80% of patients but is inadequate for the rest. For them, sinus surgery is often the best option. However, FESS is a conventional surgery that requires bone and tissue removal in order to open up blocked sinus passageways. In lieu of a desired treatment, approximately 900,000 patients each year elect to live with painful sinus conditions.
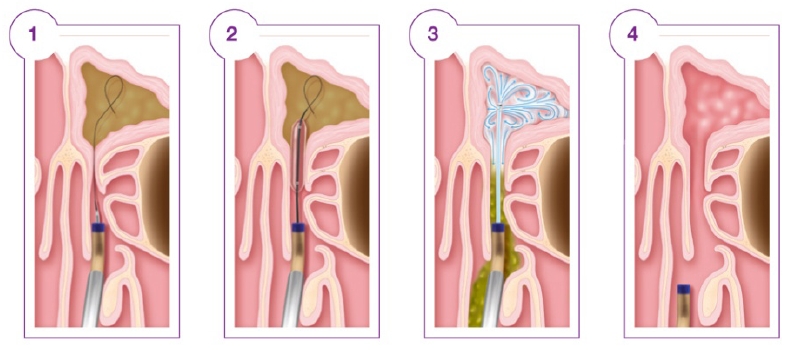
Balloon Sinuplasty of the Frontal Sinus
There is an alternative solution in endoscopic sinus surgery with the Balloon Sinuplasty™ technology by Acclarent. A small, flexible balloon catheter is placed through a nostril into the blocked sinus passageway. The balloon is then inflated to gently restructure and open the sinus passageway, restoring normal sinus drainage and function.
Drs O’Halloran and Egan have been performing Ballon Sinuplasty for over 5 years and are now offering the same procedure in the convenience of an office setting. This new technology offers a fast, safe and effective alternative to surgery or medication. Studies have shown that Balloon Sinuplasty is: